Postoperative Admission to the General Floor Reduces Hospitalization Costs in Patients Undergoing Minimally Invasive Middle Fossa Craniotomy for SSCD Repair
Medical Student Sidney Kimmel Medical College at Thomas Jefferson University
Introduction: For patients undergoing superior semicircular canal dehiscence (SSCD) repair surgery, postoperative care has traditionally been through the intensive care unit (ICU). To date, there lacks strong evidence linking ICU stay to better recovery outcomes; however, ICU stay has been associated with higher costs. Due to the minimally invasive nature of the middle fossa craniotomy, patients without significant comorbidities may be admitted to the general floor postoperatively. Here, we compare the cost data of patients admitted to the general floor or ICU for postoperative recovery and assess whether this would result in similar clinical outcomes while reducing cost.
Methods: We retrospectively reviewed the medical records of patients who underwent minimally invasive middle fossa craniotomy for SSCD repair at our institution from 2018 to 2021. Our study included 190 patients whose outcomes of interest were reported. Demographic data, SSCD laterality and characteristics, length of stay (LOS) in the ICU and/or general floor, unit charges, total visit charges, and postoperative symptoms are among the extracted variables.
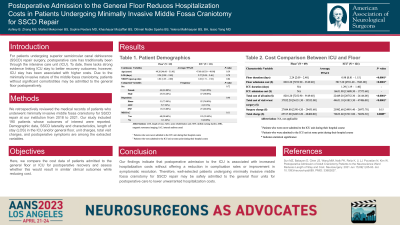
Results: The general floor and ICU cohorts included 69 and 121 patients, respectively, and were compared in terms of postoperative symptomatic resolution, complication, LOS, and unit charges. Despite patients in the general floor cohort having longer LOS (2.24 days vs 1.29 days, P < 0.0001), this cohort was significantly associated with reduced total hospitalization cost ($65 517 vs $ 70 633, P = 0.0089). Clinically, there were no significant differences in postoperative symptomatic resolutions and complications between the general floor and ICU cohorts.
Conclusion : Our findings indicate that postoperative admission to the ICU is associated with increased hospitalization costs without offering a reduction in complication rates or improvement in symptomatic resolution. Therefore, well-selected patients undergoing minimally invasive middle fossa craniotomy for SSCD repair may be safely admitted to the general floor units for postoperative care to lower unwarranted hospitalization costs.

 photo")