Clinical Research Intern Barrow Neurological Institute
Introduction: Previous studies have demonstrated the impact that race/ethnicity, socioeconomic status (SES), and health insurance have on neurosurgical outcomes, thus underscoring implicit and explicit biases that exist in the healthcare system. We analyzed the adjusted effects of these variables in patients with unruptured intracranial aneurysms (UIAs).
Methods: A retrospective analysis of all patients with UIA who underwent open microsurgery at a single center from February 2013 through December 2014 was conducted. Using the Area Deprivation Index and home addresses, patients were categorized into one of five SES tiers, where tier 1 corresponded with the least disadvantaged and tier 5 with the most disadvantaged. Firth’s logistic regression was used to perform a multivariate propensity score adjustment, using patients’ demographics, comorbidities, and postoperative aneurysm size.
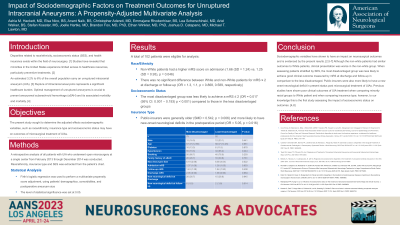
Results: A total of 102 patients were eligible for analysis. Non-White patients had a significantly higher mRS score on admission (1.66 (SD = 1.24) vs. 1.25 (SD = 0.93), p = 0.046), however, there was no significant difference between White and non-White patients for mRS ≤ 2 at discharge or follow-up (OR = 1.3, 1.1, p = 0.868, 0.589, respectively). For SES, multivariate analysis for mRS ≤ 2 at discharge showed that tier 5 patients were less likely to achieve a good outcome (OR = 0.017 (95% CI: 0.001 – 0.193) p < 0.001) compared to those in higher tiers. Public-insurers were generally older (SMD = 0.542, p = 0.006) and more likely to have new-onset neurological deficits in the postoperative period (OR = 5.05, p = 0.016).
Conclusion : We demonstrate that sociodemographic factors have an impact on clinical outcomes of UIA treatment. Of note, our patient population consisted of few Black and Hispanic patients, however, our findings highlight the need for large, multi-centered cohort studies with diverse patient populations to better substantiate the results herein.