Medical Student Robert Wood Johnson Medical School New Brunswick, New Jersey, United States
Introduction: Ethmoidal DAVFs are often associated with cortical venous drainage (CVD) and a higher incidence of hemorrhage compared to DAVFs in other locations. These may be treated with open surgical disconnection or with endovascular treatment (EVT). In this systematic review, we compare outcomes of ethmoidal DAVFs treated with open surgery versus EVT, and present three cases of ethmoidal DAVFs treated with open surgery from our institution.
Methods: A literature search was conducted between 1990 and 2021 using the PubMed and Scopus databases following the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. References were reviewed and screened by two independent authors, and disagreements were resolved through consensus.
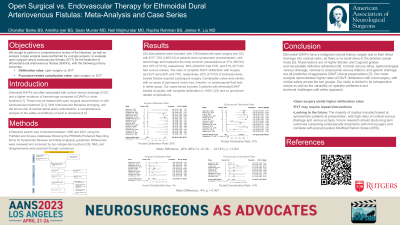
Results: 217 total patients were included. 118 patients were treated with surgery while 99 were with EVT. 70% (140/199) of patients were symptomatic at presentation, with hemorrhage being the most common presentation at 47% (93/199). 98% (202/206) had CVD, and 67% (87/132) had venous ectasia. The rates of complete DAVF obliteration with surgery and EVT were 97% (115/118) and 79% (75/95), respectively. 21% (21/99) of endovascularly-treated fistulas required subsequent surgery. 8% (10/118) of surgical cases resulted in procedure-related complications, compared to 10% (10/99) of EVT cases. Our cases series included 3 patients with ethmoidal DAVF treated surgically with complete obliteration. There were no complications.
Conclusion : Complete obliteration of ethmoidal DAVF appears to be higher with surgical intervention compared with EVT. While complications rates between the two seem similar, patients treated with EVT may require further interventions for definitive treatment. Future studies should focus on the association between venous drainage pattern and proclivity toward venous ectasia or rate of hemorrhage at presentation.

 photo")