Introduction: Gliomas pose a challenging problem as neurosurgeons must balance tumor resection with decreased morbidity. Furthermore, high-grade gliomas can penetrate eloquent areas deep subcortically, thus posing the need to identify key subcortical white matter tracts (SCWT) prior to resection. More recently, adjuncts to awake craniotomy (AC) with cortical mapping such as diffuse tensor imaging (DTI) or tractography have been used preoperatively in order to identify SCWT and assist in tumor resection planning. The purpose of this study is to elucidate the clinical effectiveness of DTI as an adjunct to intraoperative cortical mapping during glioma resection.
Methods: A literature search following PRISMA guidelines was performed using PubMed and Embase. Various combinations of search terms were used including, "awake craniotomy," "diffuse tensor imaging", "tractography" and "glioma". Variables of interest include but are not limited to: location of tumor, grade of tumor, age of operation, degree of tumor resection, and morbidity/mortality.
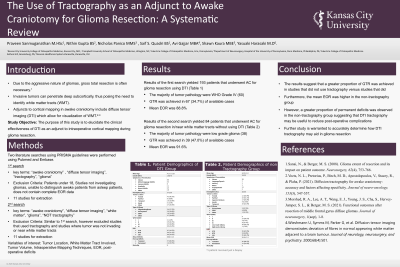
Results: After screening, results of 16 studies totaling 342 patients were included. The average age was 41. 9 ± 5.9 years consisting of 127 females. The majority of tumor pathology was WHO GRADE II (102), oligodendrogliomas (41), and were located in the left hemisphere (71.4%). Gross total resection (GTR) occurred in 143 (50.7%) of reported cases and the average extent of resection was 86.9%. Tractography results indicated tumor infiltration of SCWT in the majority of studies.
Conclusion : DTI is a viable adjunct to awake cortical mapping during tumor resection. Results indicate that studies using DTI were able to achieve GTR in half of the documented cases. Furthermore, DTI also provides information about the location of critical SCWT in proximity to the tumor, allowing for careful planning of tumor resection