Resident SUNY Upstate Syracuse, New York, United States
Introduction: CT perfusion (CTP) provides information about core infarct and salvageable tissue volume in patients with large vessel occlusion (LVO) but is not available at all institutions. We sought to evaluate whether machine learning could predict CTP parameters using patient and non-perfusion CT imaging data on presentation.
Methods: Patients who underwent MT for LVO between 2015 – 2021 at a single institution and received CTP prior to MT were reviewed. Data was divided into 80% training and 20% hold-out test sets. Hyperparameter tuning of random forest (RF) regression models was performed using random search with 5-fold cross validation. The tuned models were trained on the entire training set and tested on the test set. Models were developed to predict volume of tissue with cerebral blood flow (CBF) < 30%, tissue with time to maximum perfusion (Tmax) > 6 seconds, and mismatch volume.
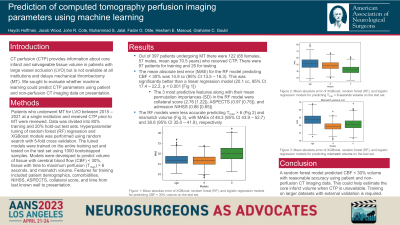
Results: Out of 397 patients undergoing MT there were 122 (65 females, 57 males, mean age 70.5 years) who received CTP. The mean absolute test error (MAE) for the RF model predicting CBF < 30% was 14.9 cc (95% CI 13.5 – 16.3). This was significantly better than a linear regression model (20.1 cc, 95% CI 17.4 – 22.2, p < 0.001). The 3 most predictive features along with their mean permutation importances (SD) in the RF model were collateral score (2.76 [1.22]), ASPECTS (0.97 [0.75]), and admission NIHSS (0.86 [0.65]). The RF models were less accurate predicting Tmax > 6 and mismatch volume, with MAEs of 48.3 (95% CI 43.9 – 52.7) and 38.8 (95% CI 35.0 – 41.9), respectively.
Conclusion : A random forest model predicted CBF < 30% volume with reasonable accuracy using patient and non-perfusion CT imaging data. This could help estimate the core infarct volume when CTP is unavailable. Training on larger datasets with external validation is required.