Introduction: Intraoperative angiography (IOA) allows visualization of neurovascular lesions intermittently during operation to confirm the obliteration of the pathology. Historically, surgeons cannulate the femoral artery at the groin, though the transradial approach (TRA) has gained momentum in recent years as an alternative providing more readily available access with fewer access site complications. Here, the authors report their experience with intraoperative angiography to compare the efficacy of these and other access sites.
Methods: Patients who underwent intraoperative angiography during neurovascular surgery at our institution over a six-year span were identified. Patient demographics, angiography details, and intraoperative and postoperative data were collected from medical records and compared over time using chi-squared test for categorical variables and t-tests for continuous variables to assess the technical outcomes and "learning curve" of IOA at these access sites.
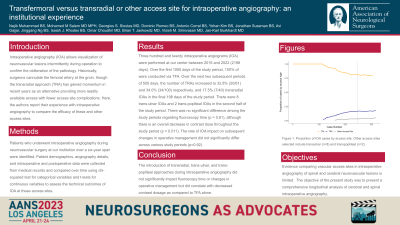
Results: Three hundred and twenty intraoperative angiograms (IOA) were performed at our center between 2016 and 2022 (2198 days). Over the first 1000 days of the study period, 100% of were conducted via TFA. Over the next two subsequent periods of 500 days, the number of TRAs increased to 32.8% (20/61) and 34.0% (34/100) respectively, and 17.5% (7/40) transradial IOAs in the final 198 days of the study period. There were 8 trans-ulnar IOAs and 2 trans-popliteal IOAs in the second half of the study period. There was no significant difference among the study periods regarding fluoroscopy time (p = 0.61), although there is an overall decrease in contrast dose throughout the study period (p = 0.011). The rate of IOA impact on subsequent changes in operative management did not significantly differ across various study periods (p=0.92).
Conclusion : The introduction of transradial, trans-ulnar, and trans-popliteal approaches during intraoperative angiography did not significantly impact fluoroscopy time or changes in operative management but did correlate with decreased contrast dosage as compared to TFA alone.