Fellow University of Illinois at Chicago Chicago, Illinois, United States
Introduction: Stroke represents a major source of morbidity and mortality in the U.S. Several large randomized controlled trials have shown efficacy of timely intervention with either intravenous thrombolysis or mechanical thrombectomy in ischemic stroke. However, most states do not have clear protocols to ensure a stroke is transported directly to a stroke center, and those with triage policies mostly occurred recently.
Methods: This cross-sectional, ecologic study utilized publicly available data. Data regarding population size, annual stroke mortality, and age-adjusted death rates resulted from the Centers for Disease Control. A listing of current certified stroke centers originated from the Joint Commission. Information on state triage policy originated from the “Get Ahead of Stroke” Campaign. States were grouped by region and by degree of policy implementation (none, some/in progress, favorable/full). One-way ANOVA and Chi-square tests were performed to assess differences in stroke mortality across regions, quantity of stroke centers, and triage policy.
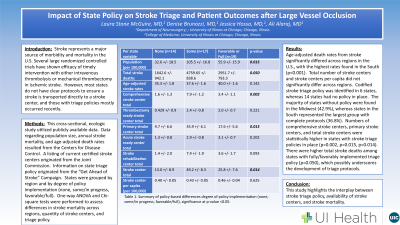
Results: Age-adjusted death rates from stroke significantly differed across regions in the U.S., with the highest rates found in the South (p < 0.001). Total number of stroke centers and stroke centers per capita did not significantly differ across regions. Codified stroke triage policy was identified in 6 states, whereas 14 states had no policy in place. The majority of states without policy were found in the Midwest (42.9%), whereas states in the South represented the largest group with complete protocols (36.8%). Numbers of comprehensive stroke centers, primary stroke centers, and total stroke centers were statistically higher in states with stroke triage policies in place (p=0.002, p=0.015, p=0.014). There was a larger population size and total stroke deaths among states with fully/favorably implemented triage policy (p=0.015, p=0.050), which possibly underscores the development of triage protocols.
Conclusion : This study highlights the interplay between stroke triage policy, availability of stroke centers, and stroke mortality.