Resident Weill Cornell Medicine New York City, New York, United States
Introduction: Encephaloceles of the lateral sphenoid sinus are rare. Originally believed to be due to defects in a patent lateral craniopharyngeal canal (“Sternberg canal”), they are now thought to originate more commonly from idiopathic intracranial hypertension, not unlike encephaloceles elsewhere in the skull base. A new classification of these encephaloceles was recently introduced, which divided them in relation to the foramen rotundum. Whether this classification can be applied to larger cohort from multiple institutions and might be useful in predicting outcome is unknown.
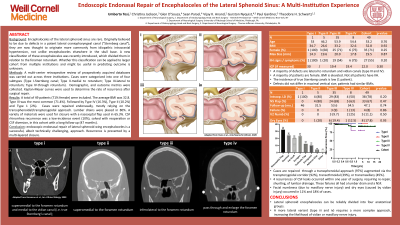
Methods: A multi-center retrospective review of prospectively acquired databases was carried out across three institutions. Cases were categorized into one of four subtypes (Type I-Sternberg canal; Type II-medial to rotundum; Type III-lateral to rotundum; Type IV-through rotundum). Demographic, and outcome metrics were collected. Kaplan-Meyer curves were used to determine the rate of recurrence after surgical repair.
Results: A total of 49 patients (71% female) were included. The average BMI was 32.8. Type III was the most common (71.4%). Followed by Type IV (16.3%), Type II (10.2%) and Type 1 (2%). Cases were repaired endonasally, mostly relying on the transsphenoidal/transpterygoidal approach. Lumbar drains were placed in 80%. A variety of materials were used for closure with a nasoseptal flap used in 65.3%. CSF rhinorrhea recurrence was a low-incidence event (10%), solved with reoperation or CSF diversion, in this cohort with a long follow-up (47 months).
Conclusion : endoscopic endonasal repair of lateral sphenoid wing encephaloceles is a successful, albeit technically challenging, approach. Recurrence is prevented by a multi-layered closure.

.jpg "Umberto Tosi, MD photo")