Medical Student University of Illinois College of Medicine Chicago, Illinois, United States
Introduction: Monitoring progress in the recovery and clinical status of patients in neurocritical care units utilizes electroencephalography (EEG) to measure brain activity, particularly for determining the effectiveness of treatment in patients with suspected seizures. While EEG monitoring varies in length from less than an hour to several days, the likelihood of detecting seizure activity with longer monitoring has not been investigated in detail.
Methods: A retrospective medical chart review of 100 adult male and female patients admitted to the neurocritical care unit at University of Illinois Hospital from 2021 was conducted. Patients selected were ordered to receive >72 hours of EEG monitoring, had no history of epilepsy, and were not pregnant. Chi-square tests and t-tests were used to analyze confirmed seizure versus length of EEG monitoring, as well as to analyze age, gender, and Glasgow Coma Score (GCS), and comorbidities. Regression analysis was performed to determine factors affecting confirmed seizure.
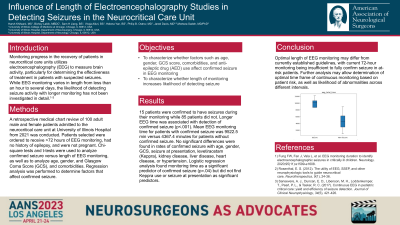
Results: 15 patients were confirmed to have seizures during their monitoring while 85 patients did not. Longer EEG time was associated with detection of confirmed seizure (p < .001). Mean EEG monitoring time for patients with confirmed seizure was 9522.5 min versus 4367.4 minutes for patients without confirmed seizure. No significant differences were found in rates of confirmed seizure with age, gender, GCS, seizure at presentation, levetiracetam (Keppra), kidney disease, liver disease, heart disease, or hypertension. Logistic regression analysis found monitoring time as a significant predictor of confirmed seizure (p=.04) but did not find Keppra use or seizure at presentation as significant predictors..
Conclusion : Optimal length of EEG monitoring may differ from currently established guidelines, with current 72 hour monitoring being insufficient to fully confirm seizure in at-risk patients. Further analysis may allow determination of optimal time frame of continuous monitoring based on patient risk, specific pathologies, as well as likelihood of abnormalities across different intervals.

 photo")