Medical Student Harvard Medical School Cambridge, Massachusetts, United States
Introduction: Magnetic resonance-guided focused ultrasound (MRgFUS) thalamotomy is a novel technique for medication-refractory essential tremor (ET). While studies demonstrate sustained improvement for up to 5 years, many report “non-responders” who lost tremor benefit after initial improvement. However, there is no standardized definition of MRgFUS failure and few comparisons of effective vs. ineffective thalamotomies to identify differentiating factors.
Methods: In this single-surgeon study, we analyzed all patients who underwent MRgFUS thalamotomy for ET from March 2016-August 2021. Using the Fahn-Tolosa-Marin tremor scoring system of the affected limb (postural + action), failure was defined as ≥50% improvement from baseline at 1 week but ≤50% at 1 year. Lesion and edema were manually outlined on 24-hour postoperative T2-weighted MRIs. Thalamic nuclei were segmented automatically using THOMAS, a multi-atlas segmentation of thalamic nuclei. The percentage volume occupied by lesion and edema was calculated for the entire thalamus and its nuclei. Logistic regression was used to assess the odds ratio (OR) per 10% increments of thalamic lesion and edema volumes, controlling for age and sex.
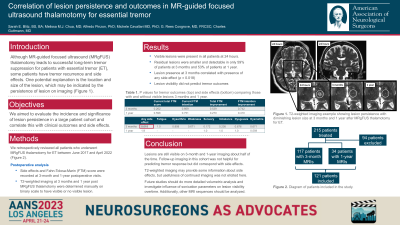
Results: Out of 129 patients, 126 had 24-hour postoperative MRIs that were analyzed. Of these, 14 (11.1%) were ineffective thalamotomies. The average±SD baseline tremor score was 7.1±2.5 with no difference in preoperative characteristics between responders and non-responders. Treatment failure was associated with relatively smaller lesion occupancy of the whole thalamus (OR=0.048, p=0.043), ventral lateral posterior (VLP) (OR=0.375, p=0.026), and ventral intermediate (VIM) nuclei (OR=0.585, p=0.018), as well as with relatively larger edema within the centromedian nucleus (CMN) (OR=1.412, p=0.043).
Conclusion : Lesions that lead to 1-year failure had less volume occupying the total thalamus and VLP and VIM thalamic nuclei as well as more edema in the CMN. Gaining insight into unsuccessful MRgFUS lesion placement can help with understanding the mechanism of failure and could influence surgical planning.

 photo")