Assistant Professor of Neurosurgery and Orthopaedics Vanderbilt University Medical Center Nashville, Tennessee, United States
Introduction: Using the Quality Outcomes Database (QOD) registry of patients undergoing cervical spine fusion surgery, we sought to: 1) determine the impact of unplanned readmission on patient-reported outcomes (PROs), and 2) compare the effect of different readmission reasons on PROs.
Methods: A multi-institution, multi-surgeon, retrospective cohort study was queried for patients undergoing cervical spine fusion surgery included in the QOD. The primary exposure was the occurrence of a 90-day unplanned readmission, which was classified into the following subcategories: medical, surgical, and pain readmissions. Other exposure variables were preoperative and perioperative data. Outcome variables consisted of the 3-12- month PROs, and included: Numeric Rating Scale (NRS)-Neck/Arm pain, Neck Disability Index (NDI), EQ-5D, and patient dissatisfaction. Multivariate logistic and linear regressions were performed.
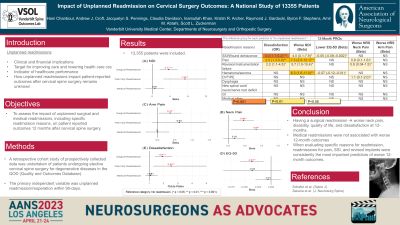
Results: Of 13,355 patients undergoing cervical spine fusion surgery, 10,897 (81.6%) underwent anterior fusion and 2458 (18.4%) underwent posterior fusion. Mean age was 56.7±11.5 and 6,594 (49.4%) were females. Unplanned readmission within 90-days of surgery was seen in 503 (3.8%) patients: medical 217 (1.6%) patients, surgical 245 (1.8%) patients, and pain 41 (0.3%) patients. Beside medical reasons, SSI/wound dehiscence was the most common reason for unplanned readmission (N=64, 12.7%). On multivariate regression analysis, surgical readmissions were associated with worse 12-month NRS-Neck pain (β=0.46,95%CI=0.15-0.77,p=0.004), NRS-Arm pain (β=0.37,95%CI=0.05-0.70,p=0.025), NDI (β=3.71,95%CI=1.73-5.69,p < 0.001), EQ-5D (β=-0.04, 95%CI=-0.06, -0.01,p=0.002), and patient dissatisfaction (OR=1.91,95%CI=1.39-2.60,p < 0.001). Pain readmissions were associated with worse 12-month NRS-Neck pain (β=0.84,95%CI=0.09-1.59,p=0.029), NDI (β=7.34,95%CI=2.55-12.13,p=0.003), and patient dissatisfaction (OR=2.53,95%CI=1.28-4.99,p=0.007). Among readmission reasons, pain, surgical site infection/wound dehiscence, hematoma/seroma, reoperations, deep vein thrombosis, and pulmonary embolism were significantly associated with worsened 12-month NRS-Neck, NDI, EQ-5D, dissatisfaction, but not NRS-Arm.
Conclusion : In patients undergoing cervical spine surgery included in the cervical module of the QOD, 90-day unplanned surgical and pain readmissions were associated with worse 12-month PROs compared to patients with medical readmissions and no readmissions.