MD/MPH Candidate Department of Neurosurgrey, Renaissance School of Medicine at Stony Brook Univiersty Stony Brook, New York, United States
Introduction: Individuals with psychiatric illness (PI) have increased rates of traumatic brain injury (TBI). Additionally, new onset PI is common after TBI; however, the influence of underlying PI on TBI outcomes is unknown.
Methods: We analyzed the medical records of 633 adult severe TBI (admission Glasgow Coma Scale (GCS) ≤8) patients admitted to our institution between 2010-2021. From medical documentation, we identified patients with previously diagnosed PI (Psych(+) cohort, n = 130) and a subset of Psych(+) patients with only SUD (SUD(+) cohort, n = 60). Patients with dementia or Parkinson’s disease were excluded (n = 24). PIs included Tourette’s syndrome, schizophrenia, obsessive compulsive, major depressive, generalized anxiety, and bipolar disorders. We compared their demographics, presentation, and outcomes to patients with no psychiatric history (Psych(-) cohort, n = 479). Primary outcome measures included discharge GCS, recovery of command following (CF), hospital length of stay (LOS), and mortality.
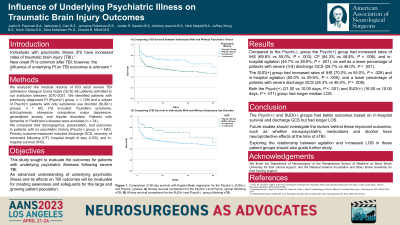
Results: Compared to the Psych(-) cohort, the Psych(+) cohort had higher rates of pedestrian trauma (21.5% vs 14.2%, P=0.031) and the SUD(+) cohort had higher rates of violent headstrike (11.7% vs 5.2%, P=0.046) as causes of TBI. The Psych(+) cohort had increased rates of survival (70.0% vs 54.9%, P=0.001) and CF (63.8% vs 48.9%, P=0.002), and fewer patients with severe (3-8) discharge GCS (28.5% vs 46.1%, P< 0.001). Furthermore, the SUD(+) cohort had increased rates of survival (70.0% vs 54.9%, P=0.017) and CF (65.0% vs 48.9%, P=0.014), and fewer patients with severe discharge GCS (28.3% vs 46.1%, P=0.006). Reciprocally, both the Psych(+) (19.50 vs 10.00 days, P< 0.001) and SUD(+) (16.00 vs 10.00 days, P=0.011) cohorts had longer LOS.
Conclusion : Patients in the Psych(+) and SUD(+) cohorts had better outcomes, but longer LOS. Future investigation should determine whether psychiatric medications have neuroprotective effects at the time of TBI or other factors explain these improved outcomes.

 photo")