Medical Student Donald and Barbara Zucker School of Medicine at Hofstra/Northwell Boyds, Maryland, United States
Introduction: Safe, maximal resection remains a modifiable prognosticator in brain tumor patients. Subcortical stimulation (SCS) is an electrophysiologic technique that allows surgeons to identify functional tracts intraoperatively to guide identification of the functional limits of surgery for peri-eloquent lesions. Current dynamic SCS devices are limited by cost and fixed cap sizes that preclude adoptability. We fashioned a novel, cost-effective dynamic SCS device utilizing an electrified conventionally available suction device with a rubber catheter and assessed its efficacy in a series of 14 brain tumor patients undergoing peri-motor tumor resections.
Methods: Consecutive patient records were retrospectively reviewed for all patients undergoing craniotomies utilizing the novel SCS device. Pre- and post-operative motor function was recorded to determine motor function preservation or deterioration postoperatively. Extent of resection and distance from the resected lesion to the precentral gyrus was characterized from magnetic resonance image scans. Lowest intraoperative SCS threshold was recorded and correlated by Fischer’s test to the presence of motor deficits and by linear regression to motor cortex proximity.
Results: Fourteen patients (12 male, 2 female) were included, with a median age of 52.5 years. The most common tumor pathology was glioblastoma multiforme (n=8, 57.1%), and the most common location was frontal lobe (n=8, 57.1%). Two patients (14.2%) suffered postoperative deficits that resolved by discharge (mean length of 7.3 days), and all other patients maintained or improved from preoperative functional status. Lowest SCS thresholds in our series were >15 mA in 6 surgeries, 10-15 mA in 3 surgeries, 5-10 mA in 3 surgeries, and < 5 mA in 2 surgeries. Lower SCS threshold was correlated to motor cortex proximity (B=1.51, p=0.001), but not to the presence of postoperative deficits (p=0.275).
Conclusion : Despite low SCS thresholds, no patients in our series suffered permanent motor deficits. Our dynamic SCS technique is inexpensive, safe, and easily adoptable.

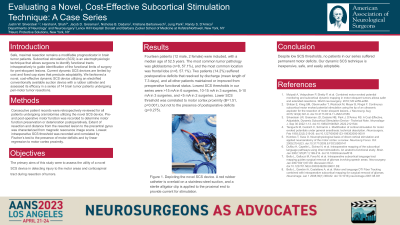
 photo")