Second Year Medical Student Florida State University College of Medicine Tallahassee, Florida, United States
Introduction: Wide-neck bifurcation aneurysms (WNBAs) pose a challenge to physicians; with safety profiles, adequate occlusion, and complete occlusion rates being suboptimal when treated with EVT. Continued innovations have provided novel systems to improve outcomes in WNBA treatment, including intrasaccular flow disrupters (Woven EndoBridge), coil-assisted aneurysm neck reconstruction devices (the PulseRider), and coil-assisted FDS (Contour and NEQSTENT systems) among others. However, complete occlusion rates at the time of treatment with these devices leave room for improvement, with rates of 71.4%, 80%, and 84.6%, respectively. Notably, none of these devices are indicated in the treatment of failed EVT.
Designed by NeuroMedica, the patent-pending BackStop represents an innovative FDS that can bridge the gap in care seen in the treatment of WNBAs with current FDA-approved devices. Specifically, WNBAs represent a high risk of recurrence and initial EVT failure. The BackStop mitigates these risks as a device designed specifically to treat these complex aneurysms when initial therapy fails.
Methods: A Biomodex model of a basilar tip wide-neck bifurcation aneurysm was printed using INVIVOTECH, a proprietary system that mimics the mechanical behavior of in vivo aneurysms by utilizing a combination of soft and rigid materials at the microscopic level. The model was placed into the Endovascular Intracranial Aneurysm Solution (EVIAS), which reproduces the body’s hemodynamics with a hydraulic system.
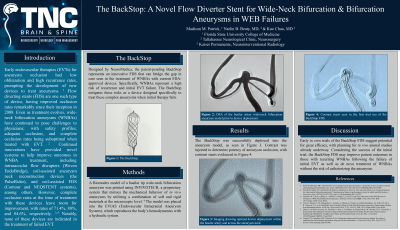
Results: The BackStop was successfully deployed into the aneurysm model. Contrast was injected to determine patency of aneurysm occlusion, with contrast stasis demonstrated.
Conclusion : Early in vitro trials of the BackStop FDS suggest potential for great efficacy, with planning for in vivo animal studies already underway. Considering the success of the initial trial, the BackStop FDS may improve patient outcomes in those with recurring WNBAs following the failure of initial EVT as well as de novo treatment of WNBAs without the risk of catheterizing the aneurysm.

.jpg "Madison M. Patrick photo")