Resident Cedars Sinai Los Angeles, California, United States
Introduction: Spontaneous subdural hematoma (SDH) is a rare form of subdural hemorrhage. Previous studies have cited mortality rates as high as 40% in elderly patients with traumatic SDH. Thus, it is imperative that we better understand how outcomes differ in elderly patients presenting with non-traumatic SDH. This study aimed to describe the clinical presentations and outcomes of patients following surgical evacuation of non-traumatic subdural hematoma.
Methods: A retrospective review of our SDH database was conducted. Patients aged 60 and greater were included who underwent surgical evacuation of a SDH between 2013 and 2021 at a single Level 1 trauma center. We used descriptive statistics to analyze patient demographics, comorbidities, complication rates, and mortality.
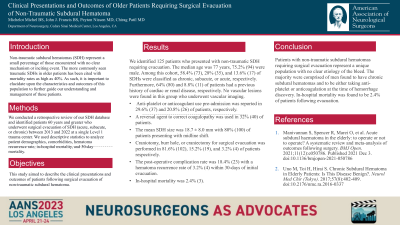
Results: We identified 125 patients who presented with non-traumatic SDH requiring evacuation. Median age was 77 years. 75.2% (94) were male. Among this cohort, 58.4% (73), 28% (35), and 13.6% (17) of SDHs were classified as chronic, subacute, or acute. Furthermore, 64% (80) and 8.8% (11) of patients had a previous history of cardiac or renal disease, respectively. Anti-platelet or anticoagulant use pre-admission was reported in 29.6% (37) and 20.8% (26) of patients respectively. A reversal agent to correct coagulopathy was used in 32% (40) of patients. The mean SDH size was 18.7 ± 8.0 mm with 80% (100) of patients presenting with midline shift. Craniotomy, burr hole, or craniectomy for surgical evacuation was performed in 81.6% (102), 15.2% (19), and 3.2% (4) of patients respectively. The post-operative complication rate was 18.4% (23) with a hematoma recurrence rate of 3.2% (4) within 30-days of initial evacuation. In-hospital mortality was 2.4% (3).
Conclusion : There is currently limited evidence regarding best management practices and outcomes in older patients with non-traumatic SDH. Our study demonstrates lower overall in-hospital mortality following surgical evacuation compared to previously reported literature.

 photo")