Postdoctoral Research Fellow Barrow Neurological Institute Phoenix, Arizona, United States
Introduction: Cavernous malformations (CM) are an uncommon intra-axial cerebrovascular disease, optimally treated via microsurgical resection. We present a cohort study of microsurgically treated cerebellar CM assessing the influence of neuroanatomic subtypes on clinical outcome.
Methods: All cerebellar CM resected by the senior surgeon from 1990-2022 were included. Variables included CM type and subtype, surgical approach, baseline and postoperative neurologic deficits, and performance status as measured by modified Rankin Score (mRS).
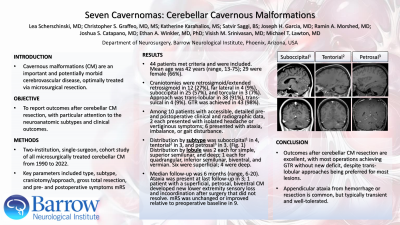
Results: Forty-four patients were eligible. Age was 42 years (range, 13-75), with a two-thirds female predominance (n=29). The surgical plan was retrosigmoid/extended retrosigmoid craniotomy for 12 (27%), far lateral for 4 (9%), midline suboccipital for 25 (57%), and torcular for 3 (7%). CM were approached via trans-lobular technique in 38 (91%), and trans-sulcal in 4 (9%). Extent-of-resection was gross total in 43 patients (98%). Detailed clinical and radiographic data were available for 10 patients, whose presenting symptoms were headache or vertigo in 2; or gait disturbance, ataxia, or imbalance in 6. Distribution by subtype was similar between suboccipital (n=4), petrosal (n=3), and tentorial (n=3). The dominant lobule was widely distributed, with representation in the simple (n=2), superior semilunar (n=2), deep (n=1), quadrangular (n=1), inferior semilunar (n=1), biventral (n=1), and vermian (n=1) lobules. CM presented to the cerebellar surface in 6, while 4 CM were deep-seated. Syndromic diagnoses were confirmed among 3 patients (33%). Overall median clinical follow-up was 6 months (range, 6-20). Most patients had no residual deficit at last follow-up; 3 demonstrated ataxia, and 1 patient reported lower extremity sensory changes and ataxia. All other patients reported stable or improved functional status (n=9, 90%).
Conclusion : Cerebellar CM outcomes are highly favorable, with almost all operations achieving gross total resection without new permanent neurological dysfunction, despite of a trans-lobular technique being widely employed. The most common deficit is appendicular ataxia, which is typically self-limited.

.jpg "Lea Scherschinski, MD photo")