Associate Consultant Apollomedics Super Speciality Hospitals, Lucknow Kolkata, WB, IN
Introduction: The study was undertaken to analyze the probable causes of recurrent AAD (Atlanto-axial-dislocation) following failed craniovertebral junction (CVJ) stabilization surgery and to help in surgical decision-making in these cases with the use of traction.
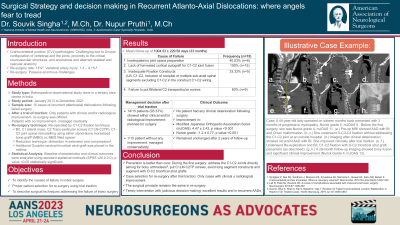
Methods: During the period from January 2013 to June December 2021, we treated 15 cases of recurrent atlantoaxial dislocations following failed surgery. After a trial of traction, they were subjected to further management. All patients, who underwent re-do surgery, were re-operated by C1-C2 fixation techniques. Their baseline characteristics and clinical outcomes were analyzed using standard statistical methods.
Results: A total of 15 patients were analyzed with a mean foillow up of 1004.53 ± 229.58 days. Inadequate/no joint space preparation(n=6, 40.03%), lack of harvested cortical autograft for C1-C2 joint fusion (n=15, 100%), inadequate fixation (U/L C1-C2, inclusion of occipital or multiple sub-axial spinal segments excluding C1-C2 in the construct C1-C2 wiring) constructs (n=5, 33.33%) and absence of Bilateral C2 transpedicular screw (n=9, 60%) were found to be the main cause of treatment failure in these cases. After trial traction, only the patients showing either clinical or radiological improvement (n=14, 93.33%) were planned for surgery. One patient who did not show any improvement was managed conservatively and he remained unchanged after 2 years of follow-up. No patient had any clinical deterioration following surgery. Mean change (improvement) in modified Japanese Orthopaedic Association Score (mJOAS: 4.47 ± 2.42, p value < 0.001 ) and Nurick grades (-1.2 ± 0.77, p value < 0.001) were statistically significant following treatment of recurrent AAD.
Conclusion : Clinical improvement following treatment of recurrent AAD without having any significant difference between clinical outcomes at the end of the first and second surgery implies that timely intervention after recognizing initial treatment failure along with judicious decision-making regarding surgical intervention can bear excellent results in recurrent AADs.