Resident Weill Cornell Medicine New York City, New York, United States
Introduction: Symptomatic ventral compression of the anterior cervicomedullary junction (CMJ) has historically been decompressed transorally. More recenty, the endonasal endoscopic odontoidectomy (EEO) has been proposed as an alternative that may permit less morbidity with earlier extubation and feeding.
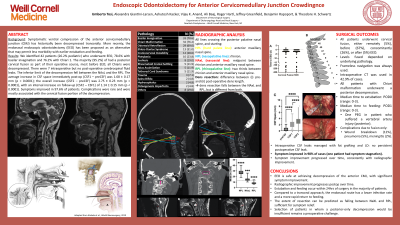
Methods: To describe the efficacy, outcomes and complications in a large series of EEO surgeries., a consecutive series of patients, prospectively entered into a database, who underwent EEO between 2011 and 2021 were studied. Demographic and outcome metrics, radiographic parameters (nasopalatine line, nasoaxial line, rhinopalatine line, extent of ventral compression) and distance (cerebrospinal fluid (CSF) space from the most posterior aspect of the compressive mass and the brainstem) were measured on the pre-(preCSF) and post-operative scans (CSF1-first scan and CSF2-most recent scan).
Results: We identified 42 patients (26.2% pediatric) who underwent EEO, 78.6% with basilar invagination and 76.2% with Chiari 1. The majority (95.2%) of had a posterior cervical fusion as part of their operative course, most before EEO; all Chiaris were decompressed. There were 7 intraoperative but no post-operative cerebrospinal fluid leaks. The inferior limit of the decompression fell between the NAxL and the RPL. The average increase in CSF space immediately post-op (CSF1 – preCSF) was 1.68 ± 0.17 mm (p < 0.0001); the overall increase (CSF2 – preCSF) was 2.75 ± 0.23 mm (p < 0.0001), with an interval increase on follow-up (CSF2 – CSF1) of 1.14 ± 0.15 mm (p < 0.0001). Symptoms improved in 97.6% of patients. Complications were rare and were mostly associated with the cervical fusion portion of the decompression.
Conclusion : EEO is safe and effective at achieving anterior CMJ decompression; it is often accompanied by posterior cervical stabilization. The decompression improves over time. EEO should be strongly considered for appropriate indications.

.jpg "Umberto Tosi, MD photo")