Fellow VCU Health Richmond, Virginia, United States
Introduction: There is strong consensus that “watertight” closure should be the goal after an incidental durotomy; however, there continues to be controversy as to how best to close the dura. Both direct and indirect repair techniques have been described in the literature and combined repair techniques are now being used to achieve watertight closure.
Methods: Medical records of consecutive patients undergoing thoracic and lumbar decompression procedures were reviewed from 2010-2020. Operative notes and progress notes were reviewed and searched to identify patients in whom incidental durotomies occurred. The specific method of dural closure was recorded. The rates of wound complications and need for revision surgery were compared with regard to the type of dural closure method used.
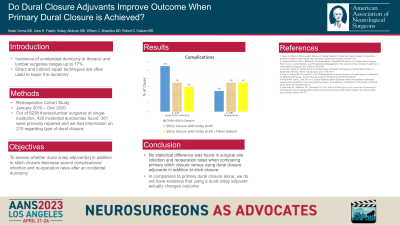
Results: We studied 210 patients, all of whom were immediately mobilized and had data available regarding the type of dural closure method used. There was no statistical difference in the rate of wound issues/infection between the group with traditional dural closure and the group where a dural onlay graft was used in addition to stitch closure (11% vs. 7%, p = 0.41) and in the rate of re-operation (5% vs. 7%, p = 0.61). Furthermore, there was no statistical difference in the rate of wound issues/infection between the group with traditional dural closure and the group where both a dural onlay graft plus a fibrin sealant was used in addition to stich closure (11% vs. 5.5%, p = 0.22) and in the rate of re-operation (5% vs. 6.9%, p = 0.60).
Conclusion : In this retrospective cohort study, the rate of wound issues and reoperation was not higher in the group where traditional method of dural closure was used. Combined repair techniques may not be necessary for every repair of incidental durotomy and traditional dural closure methods can help reduce cost.